

Preferred Retinal Locus (PRL) Assessment
California Central Visual Field Test
Mattingly Low Vision, Inc. is the sole source of the California Central Visual Field Test.
Developed by:
Donald Fletcher, MD (Primary)
Ophthalmologist,
California Medical Center,
San Francisco, CA USA
Ronald Cole, MD
Ophthalmologist,
MVT Vision Rehabilitation Center,
Sacramento, CA USA
Rebecca Kammer, OD
Chief, Low Vision Center,
Southern California College of Optometry,
Fullerton, CA USA
Produced by Mattingly Low Vision, Inc.
Escondido, CA 92026 USA
888.642.0842
www.mattinglylowvision.com
Mattingly Order Number: CCCVFT
Introduction
For many years the Fletcher Central Field Test was an inexpensive clinical tool commercially available for mapping scotoma(s) and islands of vision in the central twenty degrees of visual field. The significantly better alternative was the Scanning Laser Ophthalmoscope (SLO), but it was out of the financial reach of the majority of low vision rehabilitation practices.
As the practice of low vision rehabilitation has increasingly put an emphasis on the ability to accurately map the central field and correspondingly train the patient to effectively use their remaining vision, Drs. Don Fletcher, Ron Cole and Rebecca Kammer have worked with the original Fletcher Test and made clinical improvements to develop the new California Central Visual Field Test.
The major improvements are:
1. Several levels of brightness and size of the laser dot can be used, instead of just one, allowing more sensitivity in plotting relative scotomas that are not dense but are still clinically significant.
2. The tangent field testing form can be moved from being placed on a table between the examiner and the patient, to an upright position between the examiner and patient, allowing the examiner to better view the patient's fixation and eye movements during the test. An additional benefit is that other observers, including family members, can also see the testing results and learn about the patient's vision.
3. By using a clear upright holder for the form, the examiner can also view the laser spot on the form simultaneously with the patient. Adaptive patterns of eccentric fixation can be observed. The examiner can detect fixation losses when the patient moves fixation to the presented stimulus instead of maintaining the central reference point, and prompt the patient to direct their gaze back to the central fixation dot, allowing a more accurately plotted scotoma pattern. Alternating eye fixations may also be observed.
4. The test may be administered either monocularly or binocularly. Administration of the Test binocularly provides a functional field as used by the patient for activities of daily living as would occur in real world situations. The monocular fields are often uniquely different (a disSMARTMag® of the SLO), and may not correlate to the patient's compensatory techniques. Improved hard copy documentation of the central field can be made for insurance/reimbursement purposes.
5. Clinical observations have shown good correlation between the California Central Visual Field Test and the SLO.
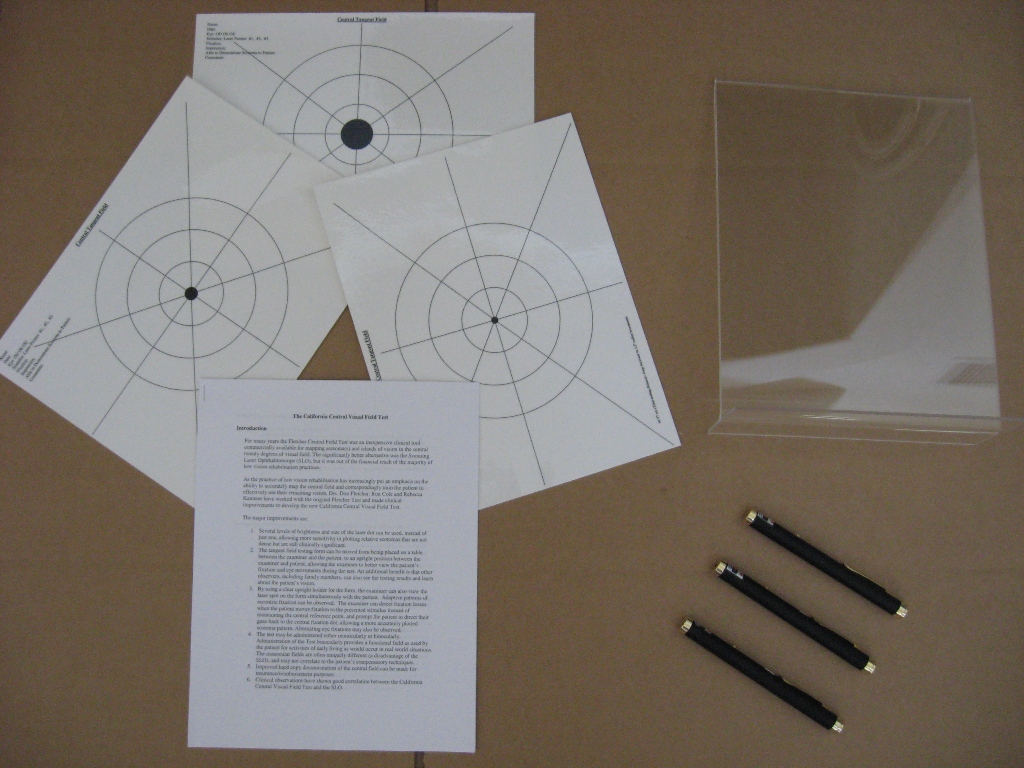
Contents of the CCVFT
1. Upright plastic tangent field form holder
2. Three unique reproducible tangent field forms (varying sized central fixation dots) for testing and scoring
3. Three unique laser pens (each has a different colored metal housing) offering three levels of brightness and size of the laser dot
4. Detailed instructions written by Drs. Fletcher, Cole and Kammer.
Indications for Using the California Central Visual Field Test
1. Suspected central field defects
2. Macular disease including age-related macular degeneration and diabetic retinopathy (ischemic maculopathy and post focal laser photocoagulation)
3. Optic neuropathies, including glaucoma
4. Difficulty with word and letter misidentification in spite of adequate magnification
5. Difficulty with page navigation (losing place, skipping lines, rereading text, etc.)
6. Slow reading that may be caused by scotomas
7. Need for education of patient in location of scotomas and compensatory eye movements to avoid scotomas
Smith-Kettlewell Reading Test (SK Read)
Smith-Kettlewell Eye Research Institute
2318 Fillmore Street
San Francisco, CA 94115
www.ski.org
Developed by:
Donald C. Fletcher, MD (Primary)
Unni Nair, MD
Manfred MacKeben, PhD
Ronald A. Schuchard, PhD
Marilyn E. Schneck, PhD
Gale Watson, MA
Published by Mattingly Low Vision, Inc.
Escondido, CA USA
Phone: 888.642.0842
www.mattinglylowvision.com
Mattingly Order Number: CSKR
Acknowledgments
- Funding to develop this test was provided in part by the Smith-Kettlewell Eye Research Institute and the Pacific Vision Foundation
- The concept of this test comes from valuable clinical experience that the authors have had with the MN Read test of Gordon Legged et al and the Pepper Visual Skills for Reading Test of Gale Watson et al.
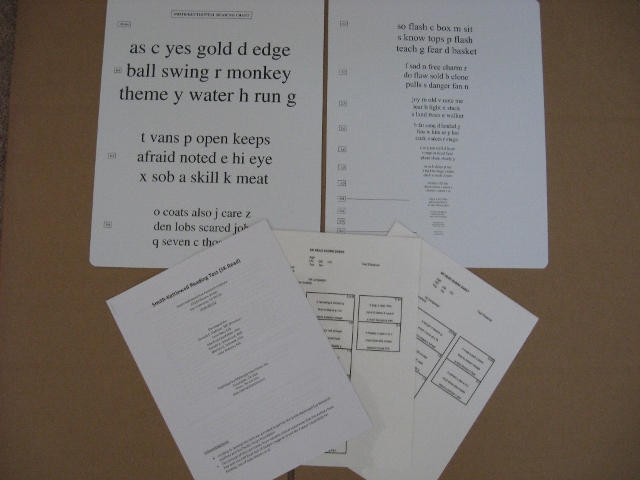
Testing Materials
- 2 SK Read Charts - version 1 and version 2 are equivalent and can be used for test retest purposes.
- Stop watch - for timing interval required to read each block of text.
- Score Sheets - have every block of text present on the test, providing space for noting mistakes to be noted and time to read each block.
- Detailed instructions for SKRead administration, scoring and integration.
Rationale for the SK Read Test
- The SK Read Test was developed to assess the reading performance of English speaking adults who may be encountering central or paracentral scotomas (visual field defects)
- The majority of patients referred for low vision rehabilitation have central visual field disruption (Reference: Fletcher, D.C.; Schuchard, R.A.: Preferred Retinal Loci (PRLs) Relationship to Macular Scotomas in a Low Vision Population, Ophthalmology, Vol. 104, Number 4, April 1997)
- Because of perceptual completion patients are frequently unaware of the presence of central scotomas, yet they affect reading performance profoundly (Reference: Fletcher, D.C.; Schuchard, R.A.; Watson, G: Relative Locations of Macular Scotomas near the PRL: Effect on Low Vision Reading; Journal of Rehabilitation Research and Development, Vol. 36, Number 4, October 1999, pp 356-364)
- The format of the MN Read Test allows it to be performed rapidly and easily. It focuses attention on impairments of resolution and is useful for determining the impact of print size on reading performance. It can be used to establish the critical print size - the smallest font where maximal rate of reading can be accomplished and is useful for estimating the response to magnification. It uses simple words in complete sentences and this tends to mask the visual field problems. When a patient has a scotoma interfere with the identification of a word, rather than verbalize an incorrect thought, they often reassess the break in context until it makes sense and then verbalize the correct wording.
- The Pepper Visual Skills for Reading Test utilizes non contextual words and is useful for identifying scotoma related mistakes. However, its format does not allow for as rapid testing with various text sizes as the MN Read format.
- The SK Read Test is designed to allow words to be easily confused and facilitate the verbalization of mistakes encountered while reading. The pattern of verbalized mistakes can help to differentiate left and right sided scotoma interference.
Characteristics of the SK Read Test
- Blocks of text range in size from 8 M units (8 times larger than 1 M newsprint) down to 0.4 M units (less than half the size of 1 M newsprint)
- Each block contains 47 letters or 60 characters including spaces. (The MN Read also has 60 characters, including spaces, per text size block)
- Each block of text contains 6 single letters, 1 two letter word, 2 three letter words, 3 four letter words, 3 five letter words, and 1 six letter word. Words were chosen from the 1000 most commonly used words in the English language.
- The use of single letters facilitates misidentification of two letter words as a single letter.
- Words that could stand alone with a letter missing from the beginning or end of the word were specifically included.
- No meaning is present in the text.
- Text is in high contrast black print on a white background.
Potential Uses of the SK Read Test
- In low vision rehabilitation clinical practice, the test can be used to identify scotomas that are interfering with reading. It is useful as a training tool to demonstrate to patients where they have a pattern of errors. It can be used pre and post training to monitor improvement in patient performance. Like the MN Read it can be used to determine critical print size and magnification requirements. The test can be used with standard reading glasses or alternately can be performed with low vision enhancement equipment.
- The test has potential application in clinical practice in general ophthalmology and particularly retinal practices. It is a useful measure of macular function that is to a significant degree independent of visual acuity. (see ARVO 2006 Nair, Fletcher, et al; SK Read Shows More Errors Than Continuous Text) Single letter visual acuity indicates the health of a very small area of the macula. This test reflects the function of a much larger area of the macula.
- The test can be utilized in research regarding any disease process that can affect the central visual field pre and post treatment as well as for rehabilitation research.